


Ear Problems and Equalising

Our ears are very important as they not only handle our ability to hear but also take care of our balance as well, so it is vitally important that we take extra care of them whilst diving as they are prone to damage if abused.
All body air spaces respond easily to the underwater world we dive in provided a diver equalises to the ambient pressure. Neglecting this crucial step, whether descending or ascending, can lead to barotrauma.
Barotrauma means injury from pressure (baro = pressure + trauma = injury).
As a diver you have a number of air spaces in and around your body that when diving, all need equalising to reduce the risk of injury. For this article, we are looking at Ear Problems and Equalising.
As divers, you will not be surprised to learn that the most frequent diving injury is some form of barotrauma to the ear. Because of the rapid relative gas volume change as the diver descends at the beginning of the dive, the first 4.2 meters of the descent is where the ear is at most risk of injury.
Anatomy of the Ear
The ear is made up of three compartments: the external ear, the middle ear and the inner ear.
The External Ear Auricle and the External Ear Canal
The auricle, is the first and most obvious view of the ear. It’s what we generally refer to as the ear, although it is just the outside section of it. Funnel-shaped and mostly cartilage covered by a thin layer of skin, it channels sound (and water) into the ear.
Directly behind the tragus, the cartilaginous prominence in front of the external opening of the ear, the ear canal curves inwards approximately 24 millimeters in the average adult. The outer portion of the ear canal contains the glands that produce earwax (cerumen). The inner portion of the ear is covered by thin, hairless skin. Pressure on this area can cause pain.
The Middle Ear
At the inner end of the ear canal, separating the external ear from the middle ear, is the tympanic membrane, or eardrum. The middle ear is an air-filled space that contains the ossicles - three tiny bones that conduct sound. Many of us learned that they are called the hammer, anvil and stirrup: but in medical terminology they are the mallus, incus, and stapes.
The Eustachian tubes, one in each ear, connect the middle ear and the back of the throat (nasopharynx). They keep the middle ear "equalised" by keeping the air pressure on both sides of the eardrum the same. Because they are surrounded by cartilaginous tissue they don’t allow for expansion.
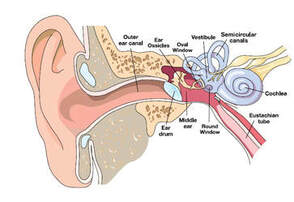
The Inner Ear
Separating the middle ear from the inner ear are two of the thinnest membranes in the human body, the round and oval windows. Damage to the round or oval windows may cause a leakage of fluid from the inner to the middle ear. This can cause a ringing or roaring in the ears, and even hearing loss. Window rupture can also cause severe vertigo and vomiting, a dangerous — even deadly — combination when underwater.
Different Types of Ear Injuries
Otitis Externa (Swimmers Ear)
This is an inflammation of the external ear caused by infection. Some people are prone to developing this kind of infection. If the ear remains moist from immersion in the water, this moisture, coupled with the warmth of the body, creates an inviting growth area for many microorganisms, especially opportunistic bacteria.
Signs & Symptoms: The ear canal can become inflamed and may partially close. The external ear canal is red and swollen and may itch. Touching the outer ear may cause intense pain and usually only one ear is affected.
Treatment: Prevention is key, especially in those persons who have previously shown they are susceptible but if left untreated, the swelling can spread to the nearby lymph nodes and cause enough pain that moving your jaw becomes uncomfortable. At this point, the only treatment is antibiotics, and diving is definitely out.
Barotitis Media (Middle Ear Barotrauma)
This is by far the most frequently reported injury among divers. People with middle ear barotrauma generally develop symptoms immediately following the dive, but delays of up to one day or longer have been reported. When the diver descends, the pressure can cause injury to the middle ear. This overpressure of the middle ear can cause serious fluid and blood to leak into the middle ear, partially or completely filling it.
Signs & Symptoms: A feeling of fullness in the ear may develop, like the feeling of fluid inside the ear. Muffled hearing or hearing loss are other indications of middle ear barotrauma. On examination with an otoscope (a special device medical personnel use when examining the ear) fluid may appear behind the tympanic membrane, causing it to bulge and appear red. In other cases, the eardrum may be retracted or sunk in. Either condition warrants immediate medical attention.
Treatment: First, diving must stop. Also, changes in altitude—as with flying—must be considered a concern as well. See a medical practitioner. The combination of over the counter / prescription drugs and time will usually allow this injury to heal in a few days, but cases have lasted up to several months. If you have been on decongestant therapy for seven days and have experienced little or no relief, it’s time to see your otolaryngologist, an ear, nose and throat (ENT) specialist.
Otitis Media (middle ear infection)
This is not a diving illness, but may look the same as middle ear barotrauma to a non-dive-trained medical practitioner. Because the treatments can vary, it is important to realise that an ear problem immediately following a dive outing usually signals a pressure-related injury rather than an infection.
Inner Ear Barotrauma: This injury generally occurs when divers attempt to forcefully equalize their ears. This "hard" blowing over-pressurises the middle ear and can result in implosive or explosive damage to the round and oval windows.
Signs & Symptoms: Vertigo, vomiting, hearing loss, loud tinnitus (a ringing or roaring sound in the ear).
Treatment: Place the injured diver in a sitting head-up position. Get the injured diver to medical help right away, preferably to someone knowledgeable in diving medicine since inner ear barotrauma may be difficult to distinguish from inner-ear decompression sickness.
Tympanic Membrane (TM) Rupture
Barotraumatic injuries to the ear may result in perforation or rupture of the tympanic membrane. This may occur in as little as 2.1 meters of water.
Signs & Symptoms: Generally there is pain and bleeding from the ear. This may not always be the case, as a number of dive-related traumatic TM ruptures have reported no pain at all. Hearing loss and tinnitus may also be present, but not always. A discharge from the ear of a clear fluid, blood or pus leakin of the ear maybe be a sign of Tumpanic Membrane Rupture
Treatment: Go to the nearest medical practitioner immediately for an examination. Do not re-enter the water if you suspect TM rupture: water entering the middle ear cavity may cause severe and violent vertigo. Do not put any drops of any kind in your ear. Do not attempt to equalise your middle ears.
External Ear Canal Superficial Vessel Rupture
This occures more often in divers who wear hoods. Occassionally, the overpressure may rupture a blood vessel inside the external ear canal, causing some minor bleeding.
Signs & Symptoms: A minute trace of blood trickling from the ear canal. Later, the injured diver may find drops of blood on his/her pillow or bedclothes.
Treatment: In order to distinguish between this injury and other, more severe injuries, it is necessary to stop diving and seek evaluation by a medical practitioner.
On a general note, a physician should examine any ear problem that drains purulent material (pus) or has a foul or disagreeable odor.
Prevention
Pressure related injuries follow failure to apply the proper procedures.
- Equalise your ears early and often - if unable to equalise then ascend slightly and reattempt to equalise. Do not equalise forcefully.. if your ears will not equalise then call it a day and have a day off diving.
- Do not dive with a cold or allergy. Use of decongestants to permit diving should be avoided.
- Ensure that none of your equipment compresses on your throat, such as a tight neck seal on your exposure suit, or the straps from a full face mask, partially obstructing the eustachian tubes. If a diver descends to far without equalising, increased air-pressure differential between the middle ear and the air in the throat may pinch eustachian tubes shut, making equalisation impossible. The most common cause of equalisation problems however, is congestion due to a cold or allergy. Mucus and swelling of the mucous membranes congest the eustachian tubes, blocking air flow to the middle ear and making it difficult or impossible to equalise.
- Do not use ear plugs and be aware that a tight fitting hood, may have to be pulled away from the ear periodically to permit normal equalisation.
- If you suffer from Swimmers Ear then consider dripping an acidic drying solution into the ear at the beginning and end of each dive day. Products such as Earol Swim (Tea Tree oil ear drops) or Swim-Seal Protective Ear Drops.
- Avoid Irritants - Cigarette smoke, exhaust fumes and exposure to allergens can increase swelling and congestion around your Eustachian tubes and make it difficult to clear. Try to breathe fresh, clean air just before a dive.
- Keep Warm - Keep yourself warm and drink a hot drink before the dive as it might help to loosen the tissues up enough for you to enjoy the dive.
- If you do have trapped water in the ear then try using Macks Dry-n-clear Ear Drying Aid. It dries and relieves the discomfort of water-clogged ears.
- Keep water out of your mask. Getting water up your nose can cause irritation to your mucus membranes, leading to an increased production of the substances that contribute to congestion.
- If wearing a hood and struggling to equalise then put your finger in your hood and pull away from your ears, this should then allow you to equalise without the pressure of the hood. Using a hole punch to punch a small hole through your hood that aligns with your ear canal can also eliminate this pressure.
Equalising
The easiest equalising technique to learn and teach, and therefore the most commonly used is the so called Valsalva Maneuver. This is the one where you exhale against a pinched nose and closed lips.
There is one problem with this method, however, it does not activate the muscles, but only presses air up the Eustachian tube. This might work as long as the tubes are kept open. If you do not equalise early enough the pressure differential might force the tissue together and hence result in closing the tube. At this point, no more equalisation is possible. If you then keep descending and forcing harder to equalise this might cause one of the injuries mentioned above.
Of most importance with any technique used that involves blowing against closed nostrils, is to blow very, very, gently and slowly. It should be a gentle constant blow. There are several other techniques scuba divers can use to equalise, like the following:
- pinch the nose and swallow or just swallow
- pinch the nose, blow and swallow
- tense your throat and push your jaw forward
- Wiggle our jaw from side to side
- close off the vocal cord, pinch your nose and make the sound of the letter “K”
There are additional tricks which can be used
- tilt your head side to side
- look up
- wiggle your jaw
- massage the tubes
- blow out of each nostril independently
- take off your mask, empty the nose, equalise, put the mask back on and clear it





